

ORIGINAL ARTICLES
Introduction. Over the past 5 years, signifi cant progress has been achieved in the treatment of patients with Ph-negative acute lymphoblastic leukemia (ALL). Treatment results were compared between two protocols of the Russian multicenter studies «ALL-2009» and «ALL-2016», in which multicomponent high-dose consolidation was not used. The principle of continuity of treatment was observed with modifi cation of doses of cytostatic drugs depending on the depth of cytopenia.
Aim – to compare the 5-year results of two studies and to determine the factors of unfavorable prognosis in the treatment of patients with ALL.
Materials and methods. The studies were performed from April 2009 to April 2016 (ALL-2009) and from April 2016 to September 2021 (ALL-2016), and 596 patients were included: 330 in ALL-2009 and 266 in ALL-2016. The analysis was performed in March 2022. The median age of patients in ALL-2009 was 28 years (15–55), in ALL-2016 – 32.5 years (18–55). Cytogenetic studies were performed in 242 patients in ALL-2009 (73.3 %) and 236 patients in ALL-2016 (88.7 %). Patients in the ALL-2016 protocol underwent a centralized assessment of minimal residual disease (MRD) by fl ow cytometry on protocol +70 day (after completion of two induction phases), +133 and +190 days. Transplantation of allogeneic stem hematopoietic cells was performed in 7 % of patients in ALL-2009 and in 9 % in ALL-2016.
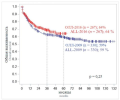
Results. Overall, relapse-free survival (OS, RFS) and the probability of relapse for a period of 3 years from the moment of inclusion of patients in a particular study were 59 %, 63 % and 23 % for ALL-2009, and for ALL-2016 – 64 %, 59 % and 22 %, respectively. For patients with B-cell precursor ALL, two cytogenetic risk groups were formed, in which long-term survival rates differed signifi cantly: the standard group (hyperploid set of chromosomes and normal karyotype) – OS 63 %, RFS 70 %, and high cytogenetic risk (any abnormal karyotype, except for hyperploidy) – OS 49 %, RFS 52 % (р = 0.001, р = 0.0014). In T-ALL, cytogenetic markers had no prognostic value, but the immunophenotype of early T-cell precursor turned out to be an important predictor of poor prognosis (the probability of relapse was 52 % compared with 15 % for all other immunophenotypic variants). According to the results of centralized monitoring of MRD, it was determined that for B-cell precursor ALL, the signifi cant negative factors are the high cytogenetic risk group and positive MRD status at +70 day, and for T-cells, the early immunophenotype and positive MRD status at +133 day.

Introduction. Optimal therapy for elderly patients with chronic lymphocytic leukemia (CLL) is the subject of intensive research.
Aim – to study the safety of obinutuzumab, as well as the selection of the optimal scheme of its use in patients with CLL, complicated by diabetes mellitus, renal insuffi ciency, cardiac comorbidity.
Materials and methods. The study included primary patients with CLL having indications requiring therapy. The inclusion criteria were: Cumulative Illness Rating Scale, CIRS) (CIRS) > 6 and or glomerular fi ltration rate (GFR) < 70 mL/min, the lower limit of GFR was not restricted. The study focused on patients with diabetes mellitus, renal failure and signifi cant cardiac pathology. Patients with Richter’s syndrome, CNS involvement, HBs-antigen, and 17p deletion were not included. In the fi rst cycle obinutuzumab was administered at a dose of 100 or 25 mg on the fi rst day and 900 or 975 mg on the second day, then at a dose of 1000 mg on days 8 and 15. For all subsequent cycles, obinutuzumab was given at a dose of 1000 mg on day 1. The dosage of chlorambucil was 10 mg/m2 from days 1 to 7. Treatment cycles in totals of 6 were repeated every 28 days.
Results. The study included 90 patients. Median age was 73.5 years, range – 60–89 years, there were 49 men (54 %) and 41 women (46 %). Twenty-four patients (27 %) had stage C, IGHV unmutated status was detected in 76 % of patients. The median creatinine clearance was 48.6 mL/min (25–110). The median CIRS score was 3 (range – 1–14). Thirty-one patients (34 %) had signifi cant cardiovascular comorbidity (previous myocardial infarction, coronary artery stenting or bypass, HF ≥ II NYHA, peripheral artery disease) as well as hemodynamically signifi cant valvular disease. Fifteen patients (17 %) had diabetes mellitus and 71 patients (79 %) had creatinine clearance < 70 ml/min. Infusion reactions to obinutuzumab grade ≥ II were reported in 29 patients (32 %). Hospitalization on the day of administration or the next day after the fi rst administration was required in 5 cases (5.5 %). Twenty-seven (30 %) patients could not complete 6 cycles. The largest number of patients (14 people, 15.5 %) stopped treatment after 1 course. The causes were the development of persistent cytopenia (n = 4), grade IV reaction to obinutuzumab (n = 3), patient’s refusal (n = 2), infectious complications (n = 2), severe tumor lysis syndrome (n = 1), acute pancreatitis (n = 1) and toxicodermia (n = 1). The leading cause of premature discontinuation on subsequent cycles was persistent neutropenia. Progression during treatment occurred in 3 patients only. Overall survival was signifi cantly predicted by CIRS (maximum discriminatory value of 3, p = 0.013) as well as GFR < 50 mL/min (p = 0.03). No other associations were identifi ed. At least 1 episode of grade III–IV neutropenia occurred in 41 % of patients. Grade IV neutropenia was associated with creatinine clearance < 60 mL/min (p = 0.05), baseline neutrophil level < 2 × 109/L (p = 0.0001), baseline monocyte level < 0.3 × 109/L (p = 0.007) and age > 70 years (p = 0.01). The effectiveness of treatment was evaluated in patients who completed at least 3 cycles of therapy. Complete remission was achieved in 26 patients (35 %), partial remission – in 41 (54 %), stabilization – in 4 (5 %), progression was noted in 3 (4 %). Sixteen patients (18 %) were not available to respond to the assessment. Minimal residual disease < 0.01 % in the bone marrow after completion of treatment was found in 17 patients (19 %), within 0.01–0.9 % – in 25 (28 %) patients. The median follow-up from the date of therapy initiation was 39.7 months (range – 0.6–72 months). The median relapse-free survival was not reached, and 2- and 3-year survival rates were 81 and 62 %, respectively. Poor relapse-free survival signifi cantly correlated with unmutated IGHV genes (HR = 2.4, 95 % CI: 1.12–5.0, p = 0.02) and partial response as opposed to complete response (HR = 3.35; 95 % CI: 1.45–7.7, p = 0.03).
Conclusion. The results of our study have practical implications as obinutuzumab is actively integrated into modern treatment regimens. Infusion reactions pose a high risk of complications in elderly patients. The dose of obinutuzumab on day 1 of administration in elderly patients, should not exceed 25 mg. The G-Clb regimen may not be optimal in patients over 75 years of age due to the unpredictable risk of complications. In patients at high risk of neutropenia, it may be appropriate to consider primary prophylaxis. ClbG is an effective regimen that resulted in high rate of MRD-negative responses and prolonged relapse-free survival.
Introduction. The new coronavirus infection COVID-19, fi rst detected at the end of 2019 in the Chinese city of Wuhan, caused a worldwide pandemic. High mortality among people with chronic diseases, a high frequency of the severe form of the disease, and an unspecifi ed number of asymptomatic carriers are all causes for heavy burden on the healthcare system, including the blood bank service.
Aim – to assess the SARS-CoV-2 antibody formation in blood donors.
Materials and methods. The research included test results for 12,314 blood samples of donors who donated blood during 04.29.2020 – 08.04.2021 at the National Medical Research Center for Hematology (Russia). Anti-RBD-SARS IgG were tested by «SARS-CoV-2-IgG-ELISA», manufactured by the National Medical Research Center for Hematology, LLC «HEMA» (Russia).
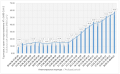
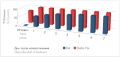
Results. Among 12,314 blood samples from donors, 3,219 (26.14 %) were positive for antibodies to SARS-CoV-2. Antibodies detection rate increased from 8.52 to 58.09 % during the observation period. For representative evaluation of donors’ anti-SARS antibodies growth profi le, the results of detection were analyzed within two-week periods (including holidays). This approach made it possible to avoid counting the same donor twice. In the profi le of the growth of collective immunity in donors, two periods were identifi ed: May – November 2020 and November 2020 – April 2021. The period of May – November 2020 proved no signifi cant change in antibodies detection in donors. Detection rate was stable at about 15 % (13.10–16.24 %). The second period, from November 2020 to April 2021, demonstrated sustainable growth of this parameter from 16.20 to 58.09 %. This is likely due to the start of the second wave of COVID-19 in Russia (starting from November 2020) and an active campaign for mass vaccination that started in December 2020. To assess the true rate of increase of specifi c immunity in donors, the frequency of primary detection of antibodies to SARS-CoV-2 in donors in relation to those donors in whom antibodies were detected earlier was analyzed. The contribution of cases of primary detection of antibodies to SARS-CoV-2 was wave-like and corresponded to the epidemiological situation.
Conclusion. An increase in the frequency of detection of antiviral antibodies in gratuitous blood donors was found during the spread of the second wave of COVID-19 and the n the beginning of mass vaccination. The increase in the overall frequency of antibody detection was due to donors with newly and re-detected antibodies. The surge in the frequency of primary detection of antibodies in blood donors corresponded to the second wave of infection.
Introduction. The concept of blood management in relation to the surgical treatment of surgical diseases recommends the correction of iron defi ciency anemia (IDA) at the prehospital stage. However, surgery is often performed for emergency indications, making it necessary to carry out treatment as soon as possible.
Aim – to evaluate the possibilities of using delta hemoglobin (Delta-He) to monitor the effectiveness of IDA therapy in neurosurgical patients at the prehospital stage to reduce the time required to prepare patients for hospitalization.
Materials and methods. A total of 42 patients were treated with high-dose iron preparations (iron [III] carboxymaltosate and iron [III] hydroxide oligoisomaltosate). During the treatment, the dynamics of the number of reticulocytes and the values of the hemoglobin delta were evaluated. Data are presented as median (IQR).
Results. Treatment with high-dose iron preparations led to an increase in Delta-He values starting from days 1–2. Significant changes were recorded by days 3–4 from the start of therapy: from 2.2 (0.3–4.9) pg to 15.5 (13.8–10) pg on day 7. These changes were 2–3 days ahead of the increase in the number of reticulocytes in the corresponding blood samples: the number of reticulocytes significantly increased by days 5–6 from the start of treatment.
Conclusion. The use of high-dose preparations of iron [III] carboxymaltosate and iron [III] hydroxide oligoisomaltosate in the form of infusion made it possible to prepare neurosurgical patients for hospitalization within a week. None of the patients required transfusion of erythrocyte-containing components of donated blood at any stage of surgical treatment. The ability to focus on Delta-He values instead of the number of reticulocytes during iron therapy made it possible to shorten the waiting period for the effect of drug exposure by 2–3 days.

Introduction. The relationship of the violation of the subpopulation composition of blood monocytes in ischemic cardiomyopathy (ICMP) with changes in monocytopoiesis, as well as the effect of colony-stimulating factor of macrophages (M-CSF) and cytokines on the differentiation of monocytes of various immunophenotypes in the bone marrow is of great relevance.
Aim – to study the role of cytokines in the mechanisms of local and distant regulation of differentiation of classical, intermediate, non-classical and transitional bone marrow monocytes in combination with the content of VEGFR2+-monocytes and hypoxia-induced factor-1a (HIF-1a) in the blood of patients with ischemic heart disease (IHD), suffering and not suffering from ischemic cardiomyopathy.
Materials and methods. Seventy-four patients with IHD, suffering and not suffering from ICMP (30 and 44 people, respectively) were examined. The number of subpopulations of classical (CD14++CD16–), intermediate (CD14++CD16+), nonclassical (CD14+CD16++) and transitional (CD14+CD16–) monocytes (in bone marrow samples) and CD14+VEGFR2+-monocytes (in blood and bone marrow) was determined by flow cytofluorimetry; the concentration of cytokines IL-10, IL-13, TNF-α, IFN-γ, M-CSF in bone marrow and blood, as well as HIF-1a in the blood, was determined by ELISA.
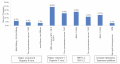
Results. Content of hematopoietins IL-10, IL-13, TNF-α, M-CSF in the bone marrow, as well as the ability of M-CSF to activate and IL-13 to inhibit the differentiation of classical monocytes from transitional cell forms were comparable between groups of patients with IHD. In the blood of patients with ICMP the concentration of IL-10 was higher, and the content of HIF-1α and CD14+VEGFR2+-cells was lower than in patients with IHD without ICMP (IL-10 – 30.00 (26.25–34.50) pg/ mL vs. 0 (23.0–28.0) pg/mL, p < 0.05; HIF-1α – 0.040 (0.029–0.053) ng/mL vs. 0.063 (0.054–0.122) ng/mL, p < 0.05; CD14+VEGFR2+ – 7.00 (5.67–7.15) % vs. 7.80 (7.23–8.17) %, p < 0.05). A feature of monocytopoiesis in ICMP compared with patients with IHD without ICMP is a high concentration of IFN-γ in the BM and a low ratio of M-CSF/IL-13 (10.00 (0.65–18.23) and 0.02 [0–0.15) pg/mL, p < 0.001; 1.02 (0.41–2.00) and 9.00 (2.13–22.09), p < 0.05, respectively), in association with a decrease in the number of classical, intermediate monocytes and an increase in the number of transitional cells in the BM in patients with ICMP relative to patients without cardiomyopathy (21.0 (19.5–23.0) and 47 (41–61.5) %, p < 0.001; 0.3 (0.0–1.2) and 18.5 (6.5–28.0) %, p < 0.01; 76.2 (73.0–78.5) and 30.5 (13.0–41.5) %, p < 0.001, respectively). At the same time, regardless of the clinical form of IHD, IL-10 and IL-13 are distant hematopoietins, TNF-α is local hematopoietin.
Conclusion. An increase in the concentration of IFN-γ and a low ratio of M-CSF/IL-13 in the bone marrow, as well as an excess of IL-10 and a lack of HIF-1a and CD14+VEGFR2+-cells in the blood of IHD patients, are associated with inhibition of differentiation of mature forms of monocytes and the development of ICMP.
Introduction. The introduction of screening testing for antibodies to the hepatitis B virus nuclear antigen (anti-HBcore) is designed to prevent the procurement of donated blood from individuals with the latent (occult) form of viral hepatitis B, in which surface HBsAg is not identified.
Aim – to evaluate the frequency of anti-HBcore markers’ occurrence in donors under the current regulatory and legal framework.
Materials and methods. This retrospective observational study was conducted with a follow-up period of one year among blood donors of the Blood Center (BC) of the Federal Medical-Biological Agency. The screening study for anti-HBcore in blood donors and its components was selective in accordance with the requirements of Appendix № 4 of Order № 1166n of October 28, 2020 of the Ministry of Health of Russia.
Results. During the study period, the BC was visited by 17,180 donors who donated blood and its components 35,840 times. There were 181 anti-HBcore tests (0.5 % of all blood samples) in 178 unique donors of blood and blood components (1.03 % of all donors). There were 14 positive, 2 questionable and 166 negative results on anti-HBcore tests. The probability of finding a positive result depending on the conditions was 9 % (7.3–14.7 %). There were no statistically significant differences in the detection of anti-HBcore in primary versus regular donors (OR = 2.539; 95% CI: 0.7321–8; p = 0.13), as well as for male donors compared with female donors (OR = 2.448; 95% CI: 0.7141–11.11; p = 0.17). 86.7 % of donors with a positive test for anti-HBcore previously had no signs of viral hepatitis B disease, the presence of questionable HBsAg was not detected, i. e. these cases may be associated with an occult form. Donors who did not previously have questionable results for various bloodborne infections during their donor career had a slightly higher probability of detecting a positive anti-HBcore test compared to donors who previously had these questionable results (OR = 1.24; 95% CI”: 0.42–3.69; p = 0.69). During the period of the donor career, 233 donations of blood and its components were made by donors with a positive result for anti-HBcore, 468 units of donor components were received, of which 365 units were given to medical institutions.
Conclusion. The probability of obtaining a positive test for anti-HBcore in the current regulatory environment is random and does not depend on the results of other infectious markers testing. It is recommended to perform anti-HBcore testing with each donation of blood and blood components.
REVIEWS

Introduction. The formation of circulating autoantibodies capable of inhibiting factors of the blood coagulation system is accompanied by the occurrence of spontaneous and/or post-traumatic bleeding in patients without a history of previous disorders of the hemostasis system. One of the reasons for the development of such conditions is acquired hemophilia.
Aim – to present algorithms for laboratory diagnosis of acquired hemophilia.
Main findings. Primary diagnosis and control of therapy of the disease are carried out based on the results of coagulation studies, the decoding and interpretation of which often causes difficulties due to the low awareness of doctors about the algorithms for laboratory diagnosis and tactics for managing patients. In acquired hemophilia there is no direct relationship between the results of laboratory tests and the clinical manifestations of the disease, which is determined by the kinetics of the interaction of autoantibodies with blood coagulation factor (F) VIII. There is a «false» in vitro decrease in the activity of factors of the internal pathway (FIX, FXI and FXII), associated with the effect of a rapid inhibitor in high titers. An important laboratory task is the determination of lupus anticoagulant, which makes it difficult to timely diagnose and verify the diagnosis.

Introduction. Currently, more and more attention is being paid to possible strategies for preventing the development of graft-versus-host disease (GVHD) and reducing the risk of infections while maintaining the antitumor effect — graft-versus-leukemia effect (GVL). In this context, the study of natural killer cells (NK-cells) seems to be quite promising.
Aim – to analyze the biological and functional properties of NK-cells after allo-HSCT, their reconstitution after transplantation and factors affecting this process, as well as the mechanisms of alloreactivity of NK cells in patients after allo-HSCT. Main findings. Various types of activating or inhibiting receptors, which are expressed on NK-cells, regulate the functions of NK-cells. Among them, the main role is played by the killer immunoglobin-like receptor (KIR-receptor), which mediates tolerance to one’s own cells and the immune response, both antitumor and directed against infectious agents. NK-cells can play a decisive role in preventing early relapses and infectious complications, as they are among the first to recover after allo-HSCT. They also have the ability to eliminate the recipient’s T-cells and antigen presenting cells (APCs), thereby preventing the development of graft failure and GVHD. There are several models of NK alloreactivity based on KIR; however, the results of studies in this area are contradictory. This review summarizes the available literature data.

Introduction. The most widely accepted notion of the function of blood clotting factor XII (FXII, Hageman factor) is its involvement in the internal blood clotting pathway. However, the biological role of FXII is diverse.
Aim – to review the diverse biological functions of FXII.
Main findings. FXII is a serine protease. The structure of FXII has a high degree of homology with plasminogen, tissue plasminogen activator and urokinase plasminogen activator. Activated FXII (FXIIa) has five substrates: high-molecular kininogen, precallikrein, FXI, plasminogen, complement proteins (C1s, C1r). FXII provides hemostatic balance by participating in the processes of blood clotting and fibrinolysis. FXII regulates inflammatory and allergic reactions by interacting with the kallikreinkinin system and the complement system. FXII has biological activity in various cells in vivo: endotheliocytes, platelets, monocytes, neutrophils, fi broblasts, dendritic cells, which determines its diverse role in physiological and pathological processes.
CASE REPORTS

Introduction. Intravascular large B-cell lymphoma is a rare variant of large B-cell, highly invasive extranodal tumors of the lymphatic system. The pathogenesis of the disease lies in the ability of tumor cells to penetrate into small vessels and capillaries of various organs. The clinical presentation is atypical for diffuse large B-cell lymphoma. In the relevant literature, information on the diagnosis and treatment of this pathology is extremely rare, therefore each publication makes a significant contribution to expanding the horizons of hematologists and morphologists.
Aim – to present a case of diagnosing intravascular B-cell lymphoma.
Main findings. A clinical case of a 78-year-old patient who fell ill acutely is presented. At the onset of the disease, febrile fever was noted. In the general blood test: hemoglobin – 104 g/L; erythrocytes – 3.0 × 1012/L; ESR – 24 mm/h; platelets – 112 × 109/L, leukocytes – 4.9 × 109/L, 4 % of cells with lymphoblast morphology were found in the leukocyte formula. Blood serum tests revealed: an increase in uric acid concentrations – up to 639 μmol/L, LDH – up to 1885 U/L, beta-2-microglobulin – up to 8.9 mmol/L, C-reactive protein – up to 0.6 g/L, a decrease in the concentration of total protein – up to 45 g/L, an increase in the concentration of aspartate aminotransferase – up to 48 units/L at normal concentrations of bilirubin and alanine aminotransferase.
The histological and immunohistochemical picture, according to the study of bone biopsy, most corresponded to bone marrow damage by intravascular large B-cell lymphoma. Immunophenotyping was carried out – 15.7 % of blast cells with immunophenotype CD19+HLA/DR+CD24+CD37+CD20+CD10+IgM+ were detected. Cytogenetic studies revealed no karyotype abnormalities. The result of fluorescence in situ hybridization of the IGH locus (14q32) was normal. Based on the data obtained, the final clinical diagnosis was established: diffuse large B-cell lymphoma, stage IVB, intravascular variant with bone marrow involvement, aggressive course. The patient was prescribed the first line of therapy according to the R-CHOP scheme (rituximab, cyclophosphamide, vincristine, prednisolone). In the control study of the bone marrow, after the first course of therapy, the number of lymphoid elements was 3.6 %, laboratory parameters returned to normal.
HISTORY OF MEDICINE
Introduction. Twenty-five years ago, on May 29, 1997, a new specialty «Transfusiology» appeared in the nomenclature of medical and pharmacological specialties, which was due to the dictates of time. By this time, blood transfusion was used in patients with various diseases in the vast majority of medical institutions. As a result of the approval of regulatory legal acts, the basis for giving the discipline an independent status was created.
Aim – to analyze the formation of the specialty «Transfusiology» in Russia.
Main findings. To conduct historical-genetic research, a set of methods was used, including research and generalization of experience, methods of monographic description and modeling, and a group of analytical methods. The sources of information were regulatory legal acts. The documents, consistently developed over two and a half decades, made it possible to formulate the duties, rights and responsibilities of a transfusiologist, as well as solve the issues of certification and postgraduate education, developed qualification characteristics, and instructions for assigning the highest, first and second qualification categories in transfusiology. Priority was given to surgeons and therapists who had the opportunity to obtain a qualification category in the specialty «Transfusiology» corresponding to their previous specialty. In 1998 the position of chief freelance transfusiology specialist was introduced. Currently, blood transfusion is offered in 38 out of 49 medical care profiles.
OBITUARY


ISSN 2411-3042 (Online)





































