

ORIGINAL ARTICLES

Introduction. Von Willebrand disease (vWD) — one of the most common coagulopathies — is characterised by a rather complicated inheritance pattern, which can be either dominant or recessive depending on the disease type. Aim. To compare clinical, coagulological and molecular genetic data obtained when examining patients with various types of vWD.
Materials and methods. The vWF gene exons were sequenced in 16 patients suffering from VWD using the Sanger method.
Results. In total, 12 various mutations were identified, one of which (Pro2527His) has not been previously observed in the world population. The c.2435delC microdeletion being a major mutation in many European countries was found to be the most common. This microdeletion was observed in 9 patients, 6 of whom had the most severe recessive form of the disease — type 3 (3 homozygotes). In two patients, this disorder was accompanied by the missense mutation Thr791Met, which allowed the authors to diagnose a rather rare recessive variant of vWD — 2N. In general, the data obtained by molecular genetic analysis correlated with the differential diagnosis of the vWD type, which is based on the clinical picture of the disease and coagulological properties. In only one case, the Arg1374Cys mutation characteristic of type 2 VWD (A/M) was observed in a patient with the alleged type 1 vWD. Most of the mutations were found in exons 18 (mainly c.2435delC deletion) and 28 which makes them the most perspective exons for the mutation search.
Conclusion. The search for mutations in the vWF gene should start from exons 18 and 28. The obtained information provides a basis for developing an economical algorithm aimed at searching for mutations in the vWF gene in our counrtry vWD patients.
Introduction. The prognosis of mantle cell lymphoma (MCL) is determined by both the intensification of the first-line therapy and the biological characteristics of the tumour.
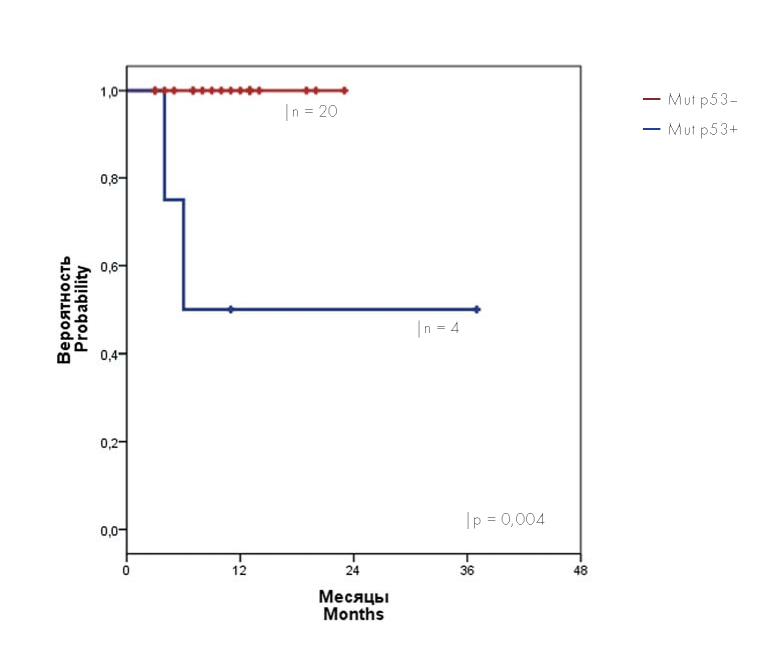
Aim. To assess the MCL incidence rate, as well as the survival rate of MCL patients with TP53 gene mutations.
Materials and methods. The prospective study MCL-2016 aimed at identifying TP53 gene mutations was carried out among 24 MCL patients from January 2016 to December 2018. TP53 gene mutations were screened using Sanger sequencing (exons 1(2)–11). No TP53 gene mutations were identified in 20 patients (20 mutp53-), with TP53 gene mutations (4 mutp53 +) being observed in 4 patients.
Results. 17 MCL patients (mut p53-) underwent two cycles of R-BAC (rituximab, bendamustine, cytarabine) and two cycles of R-HA (rituximab, cytarabine 12 g/m2 ) with the subsequent transplantation of autologous hematopoietic stem cells. Following therapy, minimum residual disease (MRD) was undetected in all 17 patients, with 3 patients still undergoing therapy. All patients, who completed the therapy, remain in complete remission with a median follow-up of 5 months following the transplantation of autologous hematopoietic stem cells (from 1 to 17 the months). The prognosis in MCL patients with TP53 gene mutations was worse. In the course of this study, two patients with TP53 gene mutations died of progressing MCL in spite of intensive therapy. In two patients with TP53 gene mutation, allogeneic hematopoietic stem cells were transplanted from unrelated completely identical donors. After undergoing the transplantation, the patients are alive and remain in complete remission (observation periods of 3 and 27 months).
Conclusion. Following R-BAC/R-HA therapy, all patients from the mutp53- group reached complete clinical and MRDnegative remission, with an acceptable toxicity profile. For MCL patients with TP53 gene mutations, the transplantation of allogeneic hematopoietic stem cells constitutes the only effective treatment.
Introduction. The intensive development of radio and electrical communications, as well as various electronic devices, leads to the electromagnetic pollution of the environment.
Aim. In this work, the authors set out to study the serum iron parameters of rats exposed to chronic electromagnetic radiation (EMR) of the decimeter range.
Materials and methods. The research was carried out on rats that were divided into experimental and control groups. The experimental group was further divided into 4 subgroups of 10 animals each, which were subsequently exposed to electromagnetic radiation at a frequency of 460 MHz (Volna-2 apparatus) for 1, 2, 3 and 4 weeks. The control group (10 rats) was exposed to pretend irradiation, with the device being turned off. The following parameters were estimated: serum iron (SI), total iron-binding capacity (TIBC) and unsaturated iron-binding capacity (UIBC) of serum, transferrin saturation (TS), as well as serum concentrations of transferrin, haptoglobin, malondialdehyde and lipid hydroperoxides.
Results. Differences in the SI concentration were found in the subgroups of animals exposed to radiation for 3 and 4 weeks (44.1 ± 3.1 μmol/l and 56.8 ± 4.4 μmol/l, respectively), as compared to the control group (30.5 ± 3.3 μmol/l). In experimental animals, TIBC increased by 41 % (p <0.05) — relative to the control group (110.8 ± 10.1 μmol/l) — only following 3 weeks of irradiation (156.2 ± 18.2 μmol/l), with a decrease in TIBC to 123.6 ± 16.4 μmol/l being noted during the 4th week. The concentration of transferrin increased from 45.6 ± 8.0 μmol/l (control) to 81.0 ± 11.5 μmol/l during the 3rd week of radiation exposure, with a decrease to 55.9 ± 6.7 μmol/l being observed during the 4th week. TS increased from 27.5 % (control) to 45.9 % only following 4 weeks of irradiation. The content of lipid hydroperoxides and malondialdehyde in the blood of irradiated rats was higher, as compared to the control animals. The serum concentration of haptoglobin amounted to 26.7 % in the control group, reaching 53.8 mg % and 47.8 mg % following 3 and 4 weeks of exposure, respectively.
Conclusion. The total chronic exposure to decimetric EMR produces an oxidising effect on organisms.

Introduction. Kidney damage at the onset of multiple myeloma (MM) is observed in 20–40 % of patients, which requires renal replacement therapy in 2–4 % of cases. Deterioration in kidney function is associated with frequent complications and a decline in the quality of life, as well as carries a high risk of early death.
Aim. To analyze the treatment of patients first diagnosed with MM, complicated by severe and dialysis-dependent renal failure.
Materials and methods. 62 MM patients with a glomerular filtration rate of <30 ml/min /1.73 m2 participated in a retrospective study (11.2014–11.2017) with the following inclusion criteria: the concentration of free light chains in blood serum being >500 mg/l and the selective nature of proteinuria. Diagnosed AL-amyloidosis served as the exclusion criterion. Depending on the need for haemodialysis, patients were divided into two groups: (I) those not requiring it (n = 16) and (II) dialysis-dependent patients (n = 46).
Results. The induction therapy included the following bortezomib-containing regimens: VCD — 41 (66.1 %), PAD — 2 (3.2 %), VD — 12 (19.4 %) and VMP — 7 (11.3 %). High-dose consolidation along with autologous hematopoietic stem cell transplantation was performed in 10 patients (16.1 %). The overall rate of anti-myeloma response in the groups came to 64.3 % (I) and 85.3 % (II) (p = 0.047), including complete and strong complete remissions in 14.3 % (I) and 14.7 % (II) of cases. The renal response was achieved by 57.2 % and 23.5 % (p = 0.032) of patients from the first and second groups, respectively. With a median follow-up of 32.1 months, throughout the entire cohort the median of progression-free survival (PFS) amounted to 14.5 months, with a 3-year PFS of 27.4 ± 6.6 %; whereas the median of overall survival (OS) came to 33.6 months, with a 3-year OS of 41.5 ± 7.7 %. There are no differences between the compared groups in terms of the survival rates. In the examined patients (n = 48), the achievement of any renal response was associated with an improvement in the 3-year PFS — 61.1 ± 11.5 % versus 17.7 ± 7.7 % (p = 0.045) — and 3-year OS — 72,2 ± 10.6 % versus 38.1 ± 10.4 % (p= 0.069). The time elapsed between the first haemodialysis procedure and the onset of anti-myeloma chemotherapy served as the predictor value of the renal response. In the group of patients who achieved a renal response, the average time came to 8.6 (95 % confidence interval of 3.5–13.7) days, as compared to 42.5 (12.6–72.5) days for patients without a renal response (p = 0.045).
Conclusion. The use of bortezomib-based regimens provides a high frequency of antitumour responses with a probability of stopping dialysis in 23.5 % of dialysis-dependent patients. Possible reasons for the low frequency of renal response include the late diagnosis of MM as a cause of kidney damage, as well as the lack of access to new anti-myeloma drugs if the induction therapy needs to be changed.
Introduction. Rotation thromboelastometry (ROTEM) is a method for studying haemostasis at the place of providing care, which allows identification of disorders on the basis of extrinsic and / or intrinsic coagulation pathways.
Aim. To study the possibility of using ROTEM for diagnosing the deficiency of individual blood coagulation factors, as well as for monitoring the efficacy and safety of haemostatic therapy in such coagulopathies.
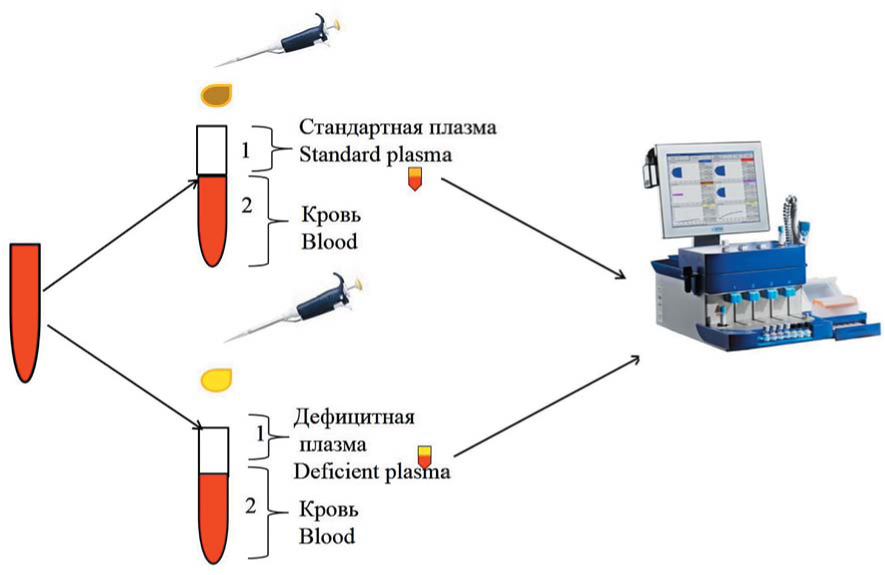
Materials and methods. The study included 9 patients with a congenital deficiency in various coagulation factors. The authors performed ROTEM, as well as coagulological tests to determine activated partial thromboplastin time, Quick’s value, fibrinogen and the plasma activity of coagulation factors FV, FVII, FVIII, FIX, FXI and FXII. In order to exclude the effects of heparin or hyperfibrinogenaemia, HEPTEM and / or FIBTEM were conducted. In order to identify the deficiency of individual coagulation factors, the authors used standard plasma samples and plasma deficient in one of the coagulation factors. The citrated blood under study was mixed with standard plasma and that deficient in one of the studied factors in a 2:1 ratio for subsequent repetition of the EXTEM and / or INTEM tests. Coagulation factor deficiency was confirmed by a change in the CT parameter.
Results. Isolated prolongation of EXTEM CT was detected in the setting of FVII deficiency; while INTEM CT prolongation occurred under the deficiency of FVIII, FIX, FXI, FXII, with simultaneous EXTEM and INTEM CT prolongation being observed in the context of FVII deficiency. The test of a mixture of citrated blood and standard plasma revealed shortened EXTEM CT in the setting of FVII deficiency and shortened INTEM CT under the deficiency of FVIII, FIX, FXI, FXII, with the shortening of both EXTEM and INTEM CT being detected in the setting of FV deficiency. In a sample containing a mixture of whole blood and plasma deficient in the studied factor, CT remained prolonged or increased. Clinical examples of using ROTEM for diagnosing coagulation factor deficiency are presented.
Conclusion. The normalisation of ROTEM parameters in a standard plasma sample along with the preservation of hypocoagulation in a factor-deficient plasma sample confirms the coagulation factor deficiency. ROTEM provides the possibility of monitoring the efficacy of haemostatic therapy for congenital deficiencies in individual blood coagulation factors.

Introduction. CD4+ Т lymphocytopenia constitutes a well-known manifestation of immune disorders in classical Hodgkin’s lymphoma (HL); however, it is not considered as a risk factor in existing prognostic models. Studies established a connection between CD4+ T-lymphocytopenia (<0.2 × 109 /l) and a pronounced reduction in the life expectancy of cancer patients.
Aim. To assess the impact of initial CD4+ T-lymphocyte deficiency in the peripheral blood on the overall survival (OS) and progression-free survival (PFS) in HL patients.
Materials and methods. The authors performed a retrospective analysis of the prognostic significance of a reduced CD4+ T-lymphocyte count in the peripheral blood prior to treatment. The analysis included 162 HL patients who had undergone combined modality therapy at the A. Tsyb Medical Radiological Research Center (2000–2016). The analysis distinguished between moderate (0.2–0.4 × 109 / l) and severe (<0.2 × 109 /l) deficiency of CD4+ T-lymphocytes.
Results. Moderate and severe CD4+ -lymphopenia was observed in 36 (22 %) and 24 (15 %) of 162 patients, respectively. The CD4+ lymphocyte count of <0.2 × 109 /l was associated with age ≥45 years (p = 0.063), advanced disease stage (p = 0.03) and international prognostic index (IPS) ≥4 (p = 0.000). With a median follow-up of 72 months, patients with an initial CD4+ T-lymphocyte count of ≤0.4 × 109 /l showed a decrease in PFS and OS, as compared to the patients without CD4+ lymphopenia. In 6 patients with CD4+ lymphopenia from the group with unfavourable stages I–II HL (n = 29), PFS came to 50 % versus 95 % (p = 0.001), and OS decreased to 40 % versus 100 % (p = 0.000). In 53 patients with CD4+ deficiency from the group with stage III–IV HL (n = 120) PFS and OS were 57 % versus 83 % (p = 0.002) and 75 % versus 98 % (p = 0.004), respectively. In 32 (34 %) patients with CD4+ deficiency from the favourable prognostic subgroup including stage III–IV HL patients with IPS 0–3 (n = 94), 5-year PFS came to 66 % versus 84 % (p = 0.037) and OS decreased to 84 % versus 100 % (p = 0.117).
Conclusion. The association of CD4+ deficiency with the treatment failure in HL patients is important in the early stages of the disease, as well as in the subgroup of patients with stages III–IV HL (IPS 0–3). The modifications of risk-adapted therapy for a small cohort of patients with an initial decrease in CD4+ seem to be justified.

Introduction. Gaucher disease (GD) belongs to the group of lysosomal storage diseases. Enzyme replacement therapy (ERT) is considered to be the current standard in GD treatment. No reduced ERT regimen has thus far been developed. Aim. To develop an optimal reduced ERT regimen for adult patients with type I GD, which is scientifically and economically viable.
Materials and methods. The study included 100 adult patients with type I GD who achieved treatment goals following at least two years of the standard ERT regimen. Patients were prescribed a reduced ERT regimen, which consisted in increasing the interval between the infusions of the recombinant enzyme up to 4 weeks, at a dose of 15–20 units/kg of body weight. The efficacy of the reduced ERT regimen was assessed once every 12 months according to main GD parameters. The follow-up period in the study ranged from 12 to 36 months.
Results. The patients with type I GD who achieved treatment goals following the standard ERT regimen and were then prescribed a reduced ERT regimen retained a stable therapeutic effect of the initial treatment according to all parameters: no clinically significant differences found in haemoglobin and platelet levels, spleen size and specific infiltration of femur bone marrow.
Conclusion. An increase in the intervals between infusions of the recombinant glucocerebrosidase up to 4 weeks for 12, 24 and 36 months did not lead to worsening of the laboratory and instrumental parameters associated with GD.
REVIEWS OF LITERATURE
Introduction. The pathogenesis of acquired aplastic anaemia (AA) is based on immune-mediated development of bone marrow failure. The absence of clear reasons for the development of immune aggression determines the relevance of investigations aimed at studying genetic disorders in the remaining pool of hematopoietic stem cells, in the hematopoietic niche, as well as mechanisms underlying the failure of immunological tolerance.
Aim. The present literature review describes the most relevant markers used for characterising AA patients on the basis of their possible response to immunosuppressive therapy (IT) and for forming groups being at risk of developing refractoriness and clonal evolution.
General findings. The overall survival probability in patients with AA following program IT is comparable to the results of transplanting allogeneic hematopoietic blood stem cells (allo-HSCT) from a related donor in the first line of therapy. According to current Russian and international recommendations, the tactics for treating AA patients is determined by the patient’s age and the presence of an HLA-identical sibling. Allo-HSCT from a related HLA-identical donor is a method used for treating patients younger than 40 years; however, the possibility of performing allo-HSCT is limited by donor availability. Although the event-free survival probability during IT is inferior to the results of allo-HSCT, IT remains the main treatment method for most patients with AA. In order to minimise adverse outcomes, it is necessary to consider predictors of treatment efficacy along with the likelihood of developing late clonal evolution as early as at the AA diagnosis stage. Patient evaluation and formation of risk groups will facilitate selection of the most optimal treatment approach at the therapy planning stage, which includes either IT combination with thrombopoietin receptor agonists, or a search for an unrelated HLA-compatible donor and timely allo-HSCT.
CASE REPORTS

Introduction. Subcutaneous panniculitis-like T-cell lymphoma (SPTCL) belongs to a rare group of skin lymphoproliferative disorders, which is characterised by panniculitis-like clinical manifestations, the α/β cytotoxic immunophenotype of tumour cells, as well as a multidirectional course from indolent to aggressive forms.
Aim. To examine patients with SPTCL having an aggressive clinical course and characterised by refractoriness to several lines of chemotherapy.
Results. We present two case reports of patients with a generalised lesions and unfavourable prognostic factors, who achieved complete long-term remission of the disease as a result of gemcitabine chemotherapy.
Conclusion. Despite the fact that both observed SPTCL patients demonstrated refractoriness to at least three types of treatment, the use of gemcitabine allowed long-term complete remissions of the disease to be achieved.
Introduction. Multiple myeloma (MM) is a lymphoproliferative disorder, for which the duration of remission is hard to predict.
Aim. To analyse the molecular genetic status of the tumour of MM patient with a short remission period at the onset and relapse of the disease, as well as to conduct its comparison with the clinical course of the disease.
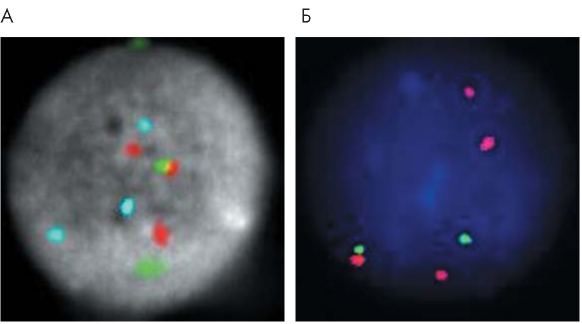
Materials and methods. Somatic mutations were detected through Sanger sequencing. The level of gene expression was analysed using RNA sequencing on the Illumina platform. In order to study chromosomal rearrangements, the authors performed fluorescence hybridisation in situ (FISH study).
Results. Prior to the treatment and during the relapse of the disease, the patient revealed a heterozygous clonal mutation p.182A>C (p.Q61P) in the N-RAS gene, which is known to hamper regulation of the MAPK signalling pathway. The transcriptome analysis performed using the RNA-seq method revealed a sharp increase in the expression of the IL6 gene during relapse (by 30 times), which could have served as a trigger for the progression of multiple myeloma, given that this cytokine stimulates cell proliferation by activating various signalling pathways (MAPK, JAK- STAT, PI3K). The progression of the disease was also accompanied by an increased expression of key regulatory genes (с-MYC, Notch2, MDM, RAF1, STAT4, mTOR) and a sharp decrease in the expression of immunoglobulin genes, which caused deep immunodeficiency in the patient. A molecular cytogenetic study (FISH) revealed trisomy of chromosomes 5, 9 and 15 at the onset of the disease. Disease relapse occurred with the amplification of the 1q21 locus, with hyperdiploidy being preserved.
Conclusion. In order to predict the duration of the remission period, a complex molecular genetic screening is required.

ISSN 2411-3042 (Online)





































