

ORIGINAL ARTICLES
Introduction. Modern therapy for relapses and resistant forms of T-cell acute lymphoblastic leukaemia/lymphoma (T-ALL/ LBL) shows poor efficacy. The use of nelarabine can improve the results of therapy in patients with refractory/relapsed T-ALL/LBL.
Aim. To evaluate the efficacy and toxicity of nelarabine treatment combined with etoposide and cyclophosphamide in adult patients with refractory/relapsed T-ALL/LBL.
Materials and methods. During the 2012–2018 period, 10 patients with refractory/relapsed T-ALL aged from 19 to 41 underwent nelarabine treatment. The patients received from 1 to 3 chemotherapy courses including nelarabine 650 mg/m2 (days 1 to 5), etoposide 100 mg/m2 and cyclophosphamide 440 mg/m2 (days 8 to 12). All the patients having achieved complete remission (СR) underwent transplantation of allogeneic haematopoietic stem cells (allo-HSCT). The development of toxic sequelae (myelosuppression, neurotoxicity, incidence of infectious complications) was considered after each chemotherapy course.
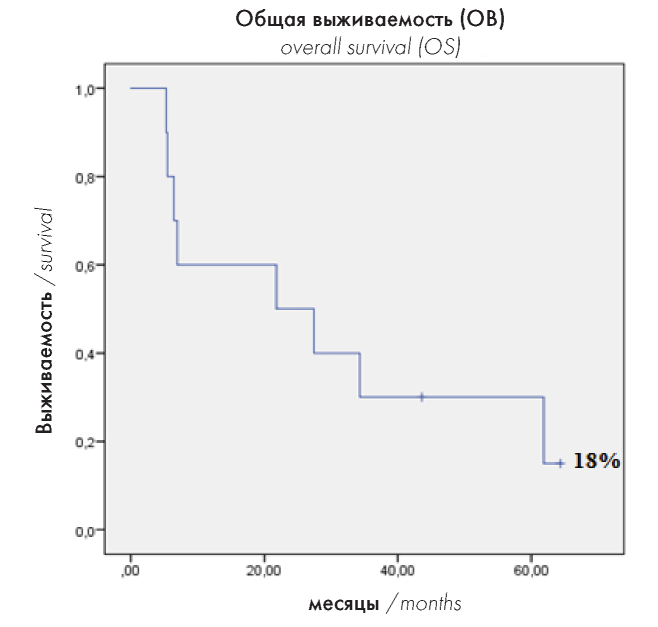
Results. Out of 10 patients who received 1–2 chemotherapy courses, 6 (60 %) achieved CR. These 6 patients subsequently underwent allo-HSCT, which was followed by early relapse in 3 (50 %) of 6 patients and the death of 1 patient in persisting CR caused by infectious complications. Only 2 of 6 patients have been monitored for 1.5 years after the allo-HSCT. The five-year overall survival rate in relapsed patients came to 18 %. In terms of toxic sequelae, myelosuppression and infectious complications were observed in all patients. Neurotoxicity was noted in 3 (30 %) out of 10 patients, with two of them experiencing it after each course and one patient — only following the third course of nelarabine treatment.
Conclusion. The use of nelarabine for the treatment of refractory/relapsed T-ALL/LBL provides the opportunity to achieve CR in 60 % of cases, as well as to perform allo-HSCT. However, long-term results are not very optimistic, thus further research is required.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship.
Introduction. The transplantation of allogeneic haematopoietic stem cells (allo-HSCT) is impossible without a central venous catheter (CVC).
Aim. To determine an optimal approach to providing venous access during allo-HSCT.
Materials and methods. This prospective, non-randomised, single-centre study included 146 patients (70 men and 76 women, median age 37 years) who underwent the first allo-HSCT. Prior to conditioning, one of the following CVCs was placed: Hickman or Leonard tunnelled double-lumen silicone catheters (BardAccessSystem); polyurethane non-tunnelled CVCs without (Certofix Duo, B. Braun) or with an antibacterial coating (Certofix Protect Duo, B. Braun). The following complications were recorded: early complications, mechanical complications, catheter-associated thrombosis (CAT), catheterrelated bloodstream infections (CRBSI), as well as catheter exit-site and tunnel infections.
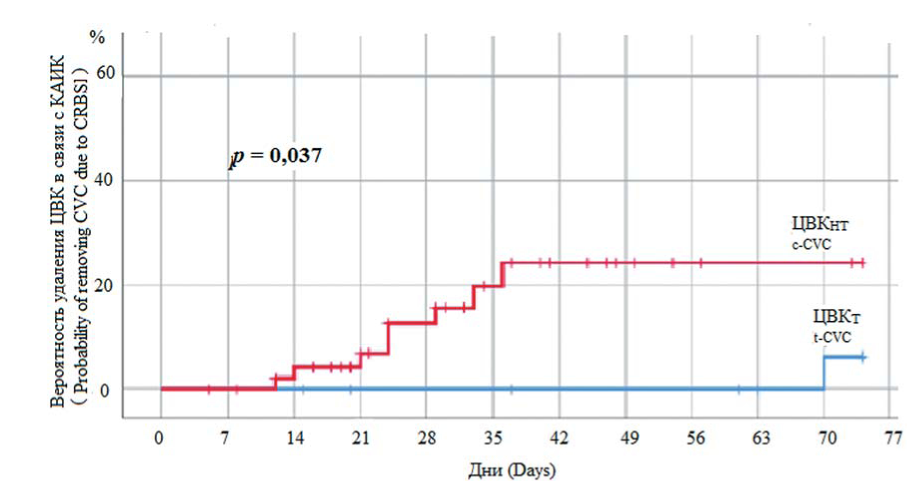
Results. A total of 320 CVCs were placed (146 prior to allo-HSCT and 174 in the post-transplant period); 259 of the CVCs were non-tunnelled and 61 were tunnelled. Non-tunnelled CVCs were used for 1–123 days (median 22 days), whereas tunnelled CVCs were implanted for 9–621 days (median 146 days). The use of non-tunnelled CVCs was associated with 2.7 % (1.0/1000 catheter days) of mechanical complications and 9 % of CAT (1.4 / 1000 catheter days). The use of tunnelled CVCs was associated with the following complications: accidental removal — 1 (1.6 %), catheter rupture — 4 (6.5 %), CAT — 5 (8.2 %) patients (0.3 / 1000 catheter days); 18 (29.5 %) patients exhibited catheter obstruction, with CVC function being restored in 14 (77.7 %) patients, whereas in 4 (22.3 %) patients the CVC was removed. The incidence of CRBSI associated with non-tunnelled and tunnelled CVCs was 4.4 and 1.5 per 1000 catheter days, respectively. The study revealed no significant differences in the probability of developing CRBSI between non-tunnelled CVCs with and without antibacterial coating (p = 0.298), as well as between non-tunnelled and tunnelled CVCs in the first 28 days after the catheter placement (p = 0.424). The risk of developing CRBSI when using tunnelled CVCs increased after 150 days of use.
Conclusion. Allo-HSCT can be performed using any CVC type. Our study revealed no advantages in employing nontunnelled CVCs with an antibacterial coating compared to those having no coating. Tunnelled CVCs (as opposed to nontunnelled ones) provide the opportunity to employ a single catheter throughout the entire transplantation and post-transplant period. It should be noted that tunnelled CVCs should not be used for more than 150 days, since prolonged use of such CVCs significantly increases the risk of infection.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship.
Introduction. Haematopoietic stem cell transplantation is the treatment of choice in many patients with malignant diseases of the blood system. In such patients, acute graft-versus-host disease (GvHD) associated with intestinal damage constitutes one of the most serious complications. However, the volume of stool per day, which is currently used as the main diagnostic criterion for such conditions, does not always permit a timely diagnosis.
Aim. To study the possibility of using intestine ultrasound examination for the diagnosis of acute intestinal GvHD.
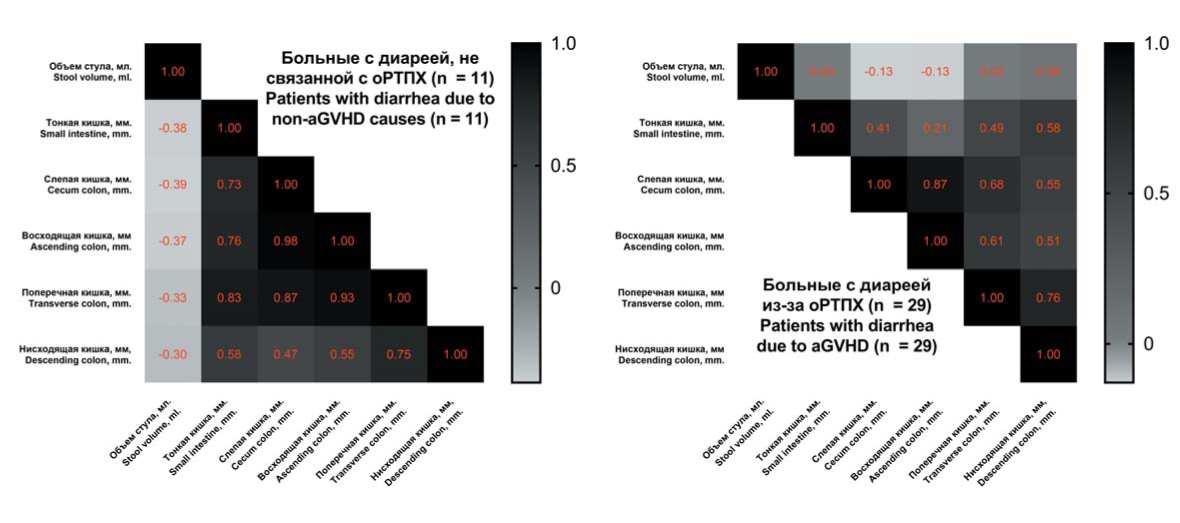
Materials and methods. The study included 50 patients having undergone transplantation of allogeneic haematopoietic stem cells, 40 of whom showed clinical signs of intestinal GvHD (diarrhoea> 500 ml/day). The control group included 10 patients who had undergone transplantation of allogeneic haematopoietic stem cells and exhibited no signs of gastrointestinal events. All patients underwent ultrasound measurement of intestinal wall thickness.
Results. Patients were divided into three groups: those with acute GvHD, those with diarrhoea of viral or infectious origin, those with diarrhoea caused by the toxic effects of chemotherapy drugs. It is shown that the walls of all intestinal sections were signifi cantly thicker in patients with acute GvHD as compared to the control group and patients with diarrhoea caused by other reasons.
Conclusion. The thickening of the caecum wall (more than 3.25 mm) as detected using the ultrasound method can be used as a diagnostic sign of intestinal GvHD.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship.
Introduction. The properties of progenitor cells in the stromal microenvironment, i.e. multipotent mesenchymal stromal cells (MMSC) and fibroblast colony-forming units (CFU-F), undergo changes in patients with chronic myelogenous leukaemia (CML).
Aim. To compare the progenitor cells of the stromal microenvironment (MMSCs and CFU-Fs) obtained from the bone marrow of CML patients at the onset of the disease, one year after the start of the treatment and during the long-term treatment with tyrosine kinase inhibitors (TKI).
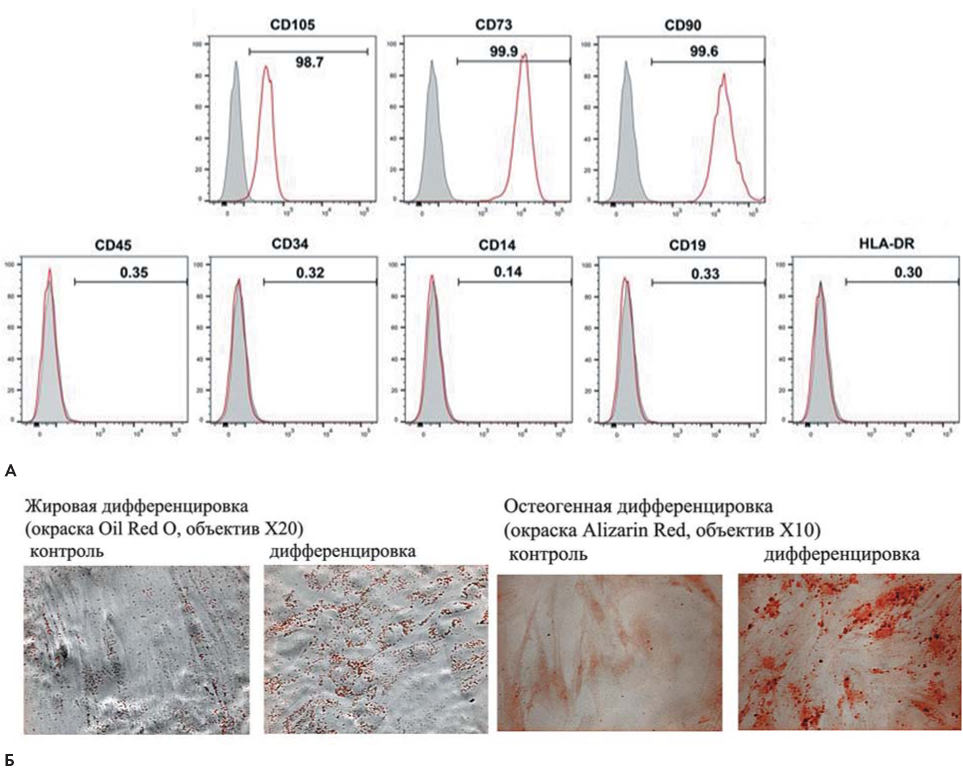
Materials and methods. The study involved an analysis of the characteristics of MMSCs, the concentration of CFU-Fs in the bone marrow of CML patients, as well as the relative expression level of genes (REL) associated with differentiation and involved in the regulation of haematopoiesis. The analysis was performed at the onset of the disease, one year after the start of the treatment, as well as 3–8 and 9–16 years after the TKI therapy. MMSCs and CFU-Fs of healthy donors were used for control purposes.
Results. The concentration of CFU-Fs at the onset of the disease did not differ from that in donors; however, the relative expression level of genes associated with differentiation was increased in the CFU-F colonies. A year after the start of TKI treatment, the concentration of CFU-Fs decreased by four times. Subsequently, the concentration increased to reach normal values following 8 years of TKI treatment. The total production of MMSCs was not changed at the onset of the disease; however, it decreased after a year of TKI treatment, subsequently returning to normal. The expression of many genes was altered in the MMSCs of patients, i.e. the REL of LIF and JAG1 increased by 10 and 2 times, respectively; in the course of treatment, the REL of LIF in MMSCs decreased, always remaining higher than in those of the donors, whereas the expression of JAG1 returned to normal. At the onset of the disease, the REL of LIF in the MMSCs of patients, who achieved a deep molecular response (DMR) within 17 months of the treatment, was three times lower than in the MMSCs of those patients who did not reach DMR within 50 months, with JAG1 not differing from that of donors.
Conclusion. Changes in stromal progenitor cells are associated with the influence of tumour cells, as well as with TKI therapy. A normal expression level of JAG1 and a decreased expression level of LIF in the MMSCs of CML patients at the onset of the disease may be predictive of DMR achievement.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship.
Introduction. Primary immune thrombocytopenia (idiopathic thrombocytopenic purpura, ITP) is a rare autoimmune disorder, whose main clinical manifestation consists in the hemorrhagic syndrome of varying severity. The therapy for ITP is aimed at eliminating hemorrhagic manifestations and maintaining patients’ quality of life. There is no information on the incidence of ITP, as well as on the clinical course and response to the treatment of ITP patients, in the Russian Federation.
Aim. To estimate the epidemiological and clinical characteristics of ITP in the adult population of the Russian Federation.
Materials and methods. We studied clinical and laboratory data derived from electronic medical records of ITP patients having participated in a multi-centre, prospective, observational, cohort study “Epidemiological and Clinical Characteristics of ITP in Adults in Russia” carried out from 2014 to 2017. The data was processed employing methods of descriptive statistics, as well as frequency analysis, event analysis and analysis of variance. The calculations were performed using the SAS V9.4 statistical package.
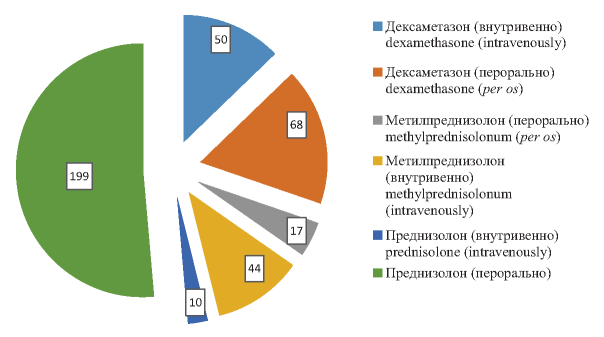
Results. The incidence of ITP in the adult population in three selected regions of the Russian Federation averaged 2.09 per 100 thousand people per year. The highest incidence rate in gender-age groups was observed in women under 40 years of age mounting to 2.7 per 100 thousand. A gradual increase in the incidence rate from 1.09 to 2.5 per 100 thousand was noted in the men over 60 years of age. A significant correlation was found between the risk of developing the hemorrhagic syndrome, its severity and the platelet count at the onset of the disease (p<0.0001). In 92.2 % of cases, glucocorticosteroid hormones were prescribed as the first line of therapy. The analysis of methods used as the second line of therapy revealed that, although splenectomy is performed relatively frequently, its likelihood has decreased from 26 to 17 % over the past three years. In addition, the proportion of patients being treated with thrombopoietin receptor agonists has increased from 5.9 to 45.7 %.
Conclusion: The incidence of ITP in three selected regions of the Russian Federation is comparable to that in other European countries.
Conflict of interest: the authors declare no conflict of interest.
Introduction. Induction chemotherapy (CT) for primary diffuse large B-cell lymphoma (DLBCL) of the central nervous system (CNS) is based on the use of methotrexate in high doses. An optimal consolidation strategy involves high-dose chemotherapy followed by autologous haematopoietic stem cell transplantation (auto-HSCT). The most effective conditioning regimen comprises a combination of chemotherapy agents including thiotepa.
Aim. To present the authors’ experience of applying auto-HSCT/TBC in patients with primary DLBCL of the CNS.
Methods. The prospective study CNS-2015 was carried out among 20 patients aged 20–52 years (median 42 years old) from 2015 to 2019. The male/female ratio came to 13/7. The somatic status of 17 (85 %) patients was 0–1 on the ECOG scale. Only 3 (15 %) patients showed the somatic status of 4 points. According to the criteria of the MSKCC prognostic system, 18 (90 %) and 2 (10 %) patients were assigned to the low-risk and medium-risk groups, respectively.
Results. All patients included in the study received 3–5 cycles of chemotherapy with high doses of methotrexate, vincristine, procarbazine and rituximab (R-MPV), as well as underwent auto-HSCT following TBC-based conditioning regimen (thiotepa, busulfan, cyclophosphamide). Prior to auto-HSCT, 15 and 5 out of 20 patients having completed induction chemotherapy achieved complete remission and partial remission, respectively. Following auto-HSCT, complete remission was achieved in 5 patients with an initial partial response to treatment. All patients underwent temozolomide maintenance therapy for 2 years. With a median follow-up of 17 (1–46) months, 18 patients are alive and in remission. Two patients, who relapsed 4 and 5 months after auto-HSCT and achieved no response to the second line of chemotherapy and radiation therapy, died 24 and 26 months after auto-HSCT.
Conclusion. R-MPV is an effective treatment for patients with primary DLBCL of CNS, which is not accompanied by severe toxicity. The use of high-dose chemotherapy with TBC allows a high remission rate to be achieved. The mortality associated with treatment in the group of patients included in the study came to 0 %.
Introduction. One of the main factors involved in the pathogenesis of burn disease consists in the disturbance of microcirculation and haemostasis, caused by increased platelet aggregation. Mechanisms underlying the enhancement of platelet aggregation are poorly understood. Main results were obtained for adult patients at the onset of the burn disease, with no similar data on paediatric patients being available. There is evidence of a relationship between the size of platelets (MPV) and their functionality.
Aim. To undertake a study of spontaneous and ADP-induced platelet aggregation and their size in children with burn disease.
Materials and methods. We studied the aggregation and size of platelets in children aged 3–17 years, in whom burn areas covered 10–70 % of the body surface at the onset of the disease and before discharge. Spontaneous platelet aggregation was analysed under conditions of induced shear flow, whereas ADP-induced aggregation was studied employing a turbidimetric method. The study of platelet sizes was carried out using a conductometric method.
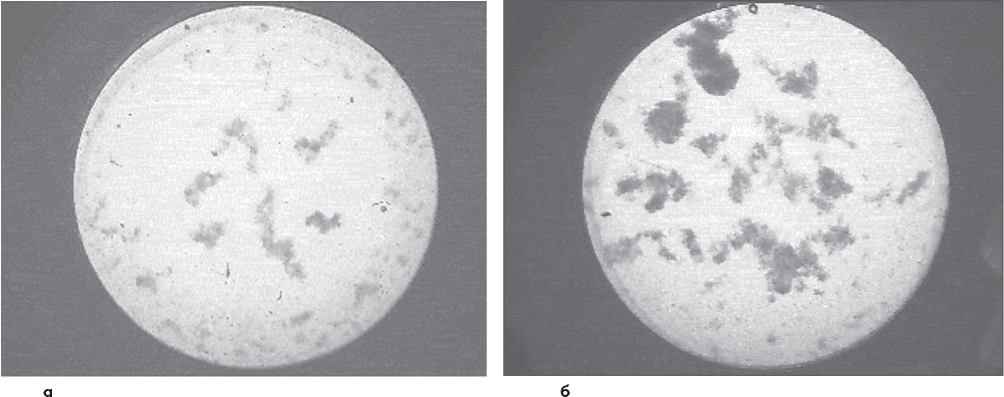
Results. Spontaneous platelet aggregation increases significantly in children with burn disease. The integrated optical density of the formed aggregates, their area and perimeter were estimated for the first time. These indicators remained elevated even after burn wounds had been completely closed. In burn disease, changes in ADP-induced platelet aggregation were multidirectional in nature. Mean platelet volume (MPV) was increased during the acute period of burn disease, decreased during the period of toxaemia, and normalised by the time of patients’ discharge. Changes in MPV did not affect the aggregation properties of platelets. There was no correlation between the degree of aggregation and the severity of hyperfibrinogenemia. The blood of burn patients contained a large number of activated platelets, which was the reason for the increase in their spontaneous aggregation, not requiring the participation of exogenous inducers.
Conclusion. An increase in spontaneous platelet aggregation was observed in children after a thermal injury, which remained elevated until the burn wounds were completely closed. A significant increase in the number of activated platelets constituted the reason for the increase in spontaneous platelet aggregation.
Conflict of interest: the authors declare no confl ict of interest.
Financial disclosure: the study had no sponsorship.
REVIEWS OF LITERATURE
Introduction. The signifi cance of ADAMTS-13 extends beyond its key role in the pathogenesis of thrombotic thrombocytopenic purpura (TTP); there is evidence of a relationship between a decrease in the ADAMTS-13 activity and thrombotic events in acute myocardial infarction and ischemic stroke.
Aim. To generalise available information on the structure and function of the metalloprotease ADAMTS-13.
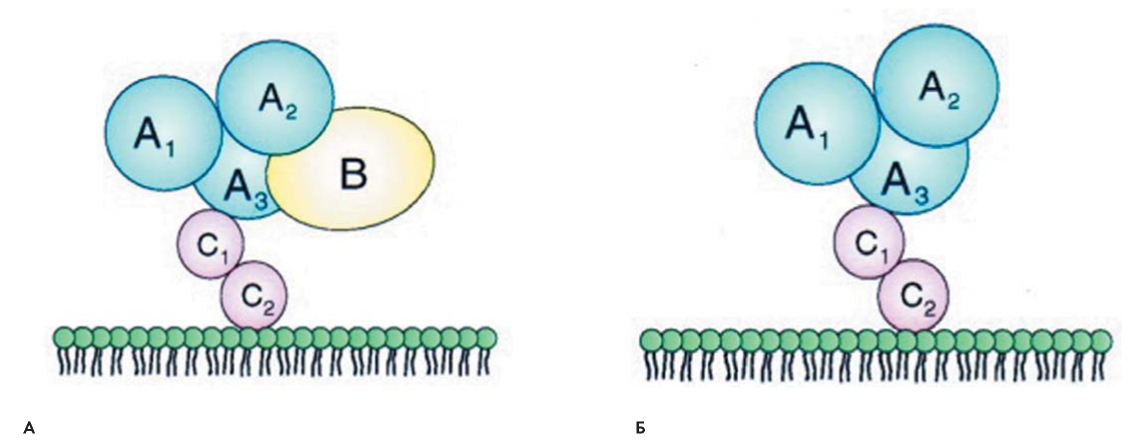
General findings. The biological function of ADAMTS-13 consists in the cleavage of ultra-large von Willebrand factor (vWF) multimers. The fact that its defi ciency causes the development of TTP provides a basis for understanding the function of vWF–cleaving protease. ADAMTS-13 has a domain structure. The functional roles of most ADAMTS-13 domains, as well as the key role of the ADAMTS-13-vWF interaction in the regulation of haemostasis, are defi ned. The conformational activation of ADAMTS-13 by vWF constitutes an important aspect of its function. After getting into the bloodstream, ultra-large vWF multimers quickly adopt a closed conformation, which becomes very resistant to ADAMTS-13 proteolysis in the absence of shear stress. Ultra-large plasma vWF multimers regain their sensitivity to ADAMTS-13 after being exposed to high fl uid shear stress, which unfolds the central vWF-A2 domain. The unfolding of a vWF molecule under shear stress conditions reveals previously hidden exosites in domain A2, which gradually increase the binding affi nity between ADAMTS-13 and vWF. The mechanism underlying the production of autoantibodies against ADAMTS-13 is unknown and requires further study. The masking of cryptic epitopes in the closed conformation of ADAMTS-13 prevents the formation of autoantibodies. Early antigen recognition of ADAMTS-13 occurs through surface-exposed epitopes in the C-terminal domains. More detailed information on the mechanisms underlying the interaction between ADAMTS-13 and the vWF can improve the understanding of mechanisms involved in the regulation of the coagulation system.
Conflict of interest: the authors declare no confl ict of interest.
Financial disclosure: the study had no sponsorship.
CASE REPORTS

Introduction. Warfarin-induced skin necrosis constitutes a rare complication of warfarin treatment.
Aim. To present a case study of the occurrence and successful treatment of atypical warfarin-induced skin necrosis in a child with congenital heart disease.
General findings. The development of finger skin necrosis in a child with congenital heart disease almost 2 years after the start of warfarin therapy was described. In addition, possible causes of the complication and methods for its treatment were discussed.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship
Introduction. Haemophilia and von Willebrand disease constitute the most common hereditary coagulopathies. However, such rare hereditary coagulopathies as congenital factor V defi ciency can mistakingly be referred to these diseases.
Aim. To describe the clinical manifestations and treatment of congenital factor V defi ciency.
General findings. The article presents a literature review, as well as three case studies of patients with congenital factor V deficiency. Given that the choice of haemostatic therapy depends on accurate diagnosis, issues associated with the differential diagnosis of hereditary coagulopathies are considered as well. Patients with congenital factor V deficiency require continuous monitoring by a haematologist in order to control spontaneous or induced haemorrhagic syndrome, as well as to plan haemostatic therapy in case of surgical procedures, pregnancy or childbirth.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship.
EXCHANGE OF EXPERIENCE
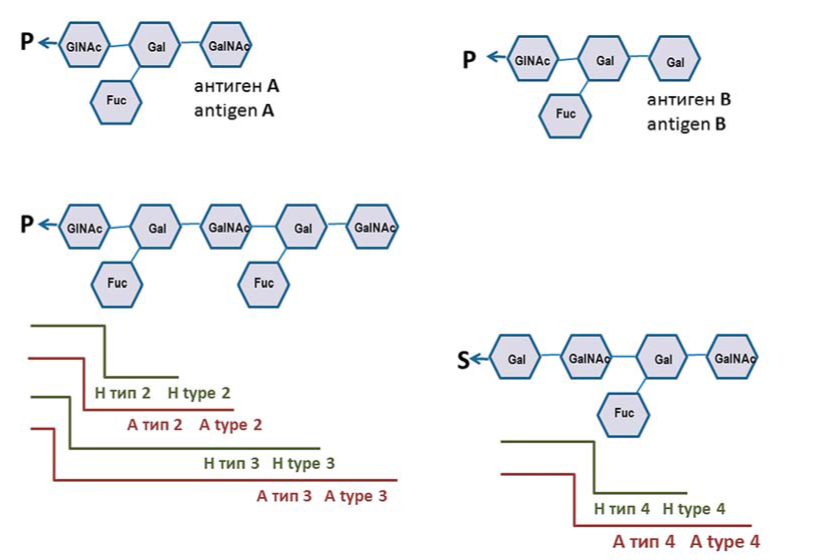
Introduction. The identification of weak variants of the A antigen, as well as their differentiation, is necessary for the proper selection of erythrocyte-containing media for blood transfusions. To this end, selective anti-A1 reagents that react only with the A1 antigen are used in combination with anti-A reagents reacting equally with the A1 and A2 antigens. Given that the expression of the A antigen varies within the subgroups and there is no established standard for reagents and procedures, the interpretation of the obtained results presents difficulties.
Aim. To develop a strategy for identifying the variants of the A antigen using available reagents in an agglutination reaction.
Methods. We compared the effectiveness of four anti-A1 and two anti-H reagents using 23 blood samples (groups A2 and A2B) and control samples (groups A1 and A1 B). Two types of anti-A1 reagents were employed: Dolychos biflorus lectin and monoclonal antibodies. All of the reagents were designed for direct agglutination reactions. Belonging of the erythrocytes to the A2 subgroup was confirmed using genetic analysis.
Results. It is shown that anti-A1 reagents did not interact with A2B red blood cells and often reacted with A2 red blood cells. The strength of the reaction with A2 red blood cells varied greatly and was weaker than with A1 red blood cells; however, it hindered the subgroup identification. Simultaneous tests conducted using an anti-H reagent allowed the authors to draw an unambiguous conclusion about blood belonging to a subgroup: a strong reaction indicated the A2 subgroup, whereas a negative or weak reaction indicated the A1 subgroup. A discrepancy was noted between the results obtained for two donors using serological and molecular methods: the A3 subgroup was identified serologically, whereas genotyping revealed the AB0*A1 allele. In both cases, direct sequencing showed a combination of mutant alleles giving the A3 phenotype. When using commercial kits to perform genotyping analysis through a polymerase chain reaction, it should be taken into consideration that primers are matched to the most common variants and cannot detect all mutations of the AB0 gene.
Conclusion. Reliable identification of the A2 subgroup through serological methods is possible when using lectin or monoclonal anti-A1 antibodies in combination with a monoclonal anti-H reagent.
Conflict of interest: the authors declare no conflict of interest.
Financial disclosure: the study had no sponsorship.

ISSN 2411-3042 (Online)





































